

In 1962, in Seattle, USA, Dr. Belding Scribner began the hemodialysis treatment that would allow treating patients with chronic kidney failure (CKF), which cannot filter their own blood. Scribner created a connector, between the dialysis machine (blood purifier) and the patients, and the teflon arteriovenous cannula, in 1961 (1). Unsurprisingly, the machines were insufficient for the number of patients who needed to be dialyzed. Therefore, a committee was created to decide which patients would receive treatment.
A group of professionals from different areas had to decide together whether a patient received or not the treatment, after the doctors carried out the first clinical filter and pre-selected the patients suitable to be dialysed. The committee was known as the God Committee, since it somehow decides who lives.

The "God Committee"
Life magazine published an article dedicated to the committee entitled “They decide who lives and who dies”, written by Shana Alexander. The article tells the story of one treated patient that survived due to the treatment, and also tells the committee’s story. The article included a profile of each member of the committee and a photo of the group, with their faces ominously shadowed:
“These seven citizens are in fact a Life or Death Committee. With no moral or ethical guidelines but their own individual consciences, they must decide, in the words of the ancient Hebrew prayer, ‘Who shall live and who shall die; who shall attain the measure of man’s days and who shall not attain it; who shall be at ease and who shall be afflicted’”(3)
This kind of decision-making during complex or critical situations, although disturbing, is not uncommon. In these contexts, we must fairly distribute (equity) a common good (healthcare) with limited resources. This common good is also a fundamental human right and it is considered essential for societal progress and the strengthening of human dignity. Healthcare is not centered only on diseases and treatment, but prevention, promotion and protection of health. These tasks implies a political commitment based on the ethical principle of justice. (4)
In the scope of healthcare, ethical decisions are permanent. It might be easier for us to see them in matters of social debate on topics such as abortion, embryonic selection, euthanasia, surrogate motherhood, genetic manipulation, and eugenics. However, they are part of all clinical actions and today, in the pandemic context, we face profound reflections and ethical decision-making. Healthcare professionals will answer questions such as: Who will access treatment or use the intensive care unit (ICU) beds, if we face scarcity? What commitments (moral imperative) should the healthcare personnel assume at the expense of their own or their family’s health? How surveillance, quarantine, and social distancing should be implemented considering the ethical norms, human rights and civil liberties? What obligations and responsibilities do countries have to plan and join the efforts to face the pandemic?
On March sixth, the reason of the Italian government’s delayed response to the Covid-19 pandemic, according to expert opinion, was the development of an ethical guideline by the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Therapy (ISAARIT). The ethical recommendations of this guideline addresses admission of patients into the ICU, and cessation of care. The guideline takes into account the exceptional unbalance between needs (number of infected patients and their requirements) and available resources (number of ICU beds, ventilators, and trained staff to provide safe care).
This seven-page guideline begins by stating, that in addition to the clinical adequacy criteria (that the patient requires the treatment) and the proporcionality (balance between the base disease, the general condition, and the prognosis of the patient (6)), it is necessary to consider distributive justice and the appropriate use of scarce healthcare resources. The use of triage, a structured system that guarantees the patient’s attention according to the disease severity, prioritizes the patient’s attention assuring that those labeled as urgent or in critical condition receive care first.
Who will first receive care during a global emergency such as a pandemia? This is a tough question, but “if these questions are not taken into account during planning, the response efforts could be severely diminished during the pandemia. A publicly discussed ethical framework is critical to uphold public trust, promote compliance/enforcement and reduce the social disruption, and the financial losses”
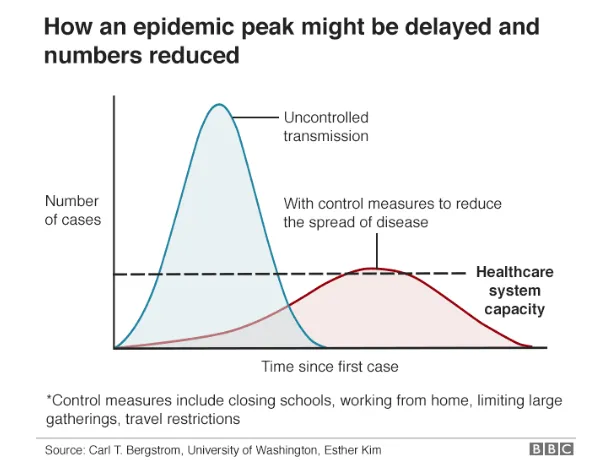
Reflections as the mentioned above are fundamental, because we’ll be facing these kinds of moral decisions, as today we find ourselves in the urgency of flattening the curve. Flattening the curve, to avoid a critical mass of infected patients at the same time and for slowing the spread of the disease, is the strategy to avoid the collapse of our health system, and might be one option to not rescind care of patients.
The moral decisions, opposed to what many might think, are not gut or intuitional decisions, nor based on a doctor's personal beliefs. These decisions must be deliberated on a case by case basis (condition’s severity, chronic disease, deterioration of other systems, possibilities of reversibility, patient’s wishes, advance care directives, etc) and also on our own societal values.
Italy made its own decisions, where intensive care treatments are guaranteed to patients with greater possibilities of therapeutic success. Therefore, a patient with "greater life expectancy" will receive the privilege of care.
This is based on a utilitarian decision-making criterion of "the greatest benefit, for the greatest number of people". So, access to intensive care in a context of extreme imbalance of distributive justice between request and availability (supply and demand), justified by an extraordinary situation. In other words, when not all the patients who need treatment can be treated, it is necessary to choose which patients to attend.
The guideline and the decisions that follow from the recommendations, have caused much stir and public questioning, and some of the following questions rightfully arise: What will happen to the infected older adults? (Among the Italian options is to establish an age-limit for admissions to the ICU in order to reserve the scarce resources for those with a higher likelihood of survival and life expectancy) What will happen to the infected chronic patients? What will happen to the infected advanced cancer patients?
These questions appear when the utilitarian principle “saving the maximum number of lives” collides with the equity principle, which refers to a fair distribution of benefits and burdens. Sometimes, it may be considered fair that the distribution be equal between the subjects, while some other times it may be considered fair that the distribution be in accordance with the needs of the people - to give preference to those who by their conditions are in decline the poorest, the sickest, most vulnerable.
Are we aware of the situations we will experience if our health system collapses? Do we realize the importance of flattening the curve?
The World Health Organization (WHO) proposes general considerations for those that are responsible for developing their country’s public policies. The process must include setting priorities and promoting equitable access. That involves civil society and other stakeholders, so that the decision-making regarding resource allocation is transparent and inclusive. On the other hand, it establishes that this process must incorporate clear and pre-established mechanisms to review the agreement decisions, when new data becomes available.
This point is particularly relevant since death, dying and end-of-life processes are usually not present in conversations, neither within families, healthcare professionals or the mass media. There is often confusion between withdrawal or withholding of a treatment, rejection of a treatment, abandonment ("let die"), terminal sedation, and euthanasia (6), which in the context of a pandemic may cause more fear-mongering and feelings of anger, untrust and injustice.
Communicates about medical decisions to be taken in these contexts and its ethical foundation, should be part of the public policy of confronting the pandemic.
As for the prioritization criteria, we saw that the utilitarian logic can send shivers when a particular case hits news headlines (and certainly, unleashes a scandal). But the prioritization criteria has an ethical-evidence based framework, based on saving as many people as possible. Policy and decision-makers should consider this ethical framework when defining policies. However, we can not leave out the analysis of equity considerations, from which priority can be given to those in more critical condition due to the disease, and to vulnerable and disabled populations .
One point under discussion is age, which has been the most controversial of the criteria defined in the document published by the ISAARIT. While it is considered fair to give an opportunity to younger people and reduce their global burden of disease (7), it is debated whether there is age discrimination. It has been shown that having advanced age worsens the prognosis of any measure, so seeing it exclusively from the probabilistic point of view, the decision to exclude older people seems reasonable.
Those who question this position wonder if these decisions define the values of a society, then what value do our older adults have in society? They provided their care and work for decades, and now they are in need of assistance. Should we abandon them? However, let's not forget that in this scenario, we will always be leaving someone without the required attention.
In this complex health crisis scenario, full of uncertainty and scarce resources, the ethical reflection and deliberation is key to decision making. This process must be shared, not only with other healthcare professionals, but also through permanent communication with the patient and their family. Although case by case analysis is important, the development of guidelines for these situations allows guiding the clinician’s action, and that the burden of the moral-decision does not fall on professionals as sole actors.
What is or will be the ethical guideline of our health system?
Even in a crisis context such as this, the health system must guarantee the care for all populations regardless their chance of survival or age, but based on the particular needs for all kinds of patients. For those patients who do not have the same chance of survival as younger people, but also for those in the process of “withhold and withdraw treatment”. It is a must to assure that these patients always receive alleviation for their pain and suffering (palliative care). Actually, in a health emergency situation, it is imperative to allocate human and financial resources to achieve this goal. These patients and their families are at great risk of feeling abandoned by the health system, and should not be denied care. That makes sense to the fact that while there will be groups that do not need intensive care criteria, we must ensure that they receive high quality palliative care. It is our duty to ensure that health systems go along with these patients and do not abandon them, and if possible, to let them die painlessly and in peace.
Preparing for this scenario is an ethical imperative.
1.
Lolas, F. (1997). Bioética: Una Palabra con Historia. El Mercurio. Recuperado de: https://uchile.cl/u76968
2.
Pose, C. (2016). Los inicios de la consultoría ética: los comités de ética y su constitución. A Fondo, 29.
3.
Alexander, S. (1962). They decide who lives, who dies. Life, November 9, 102-125.
4.
Penchaszadeh, V. (2018). Bioética y salud pública. Revista Iberoamericana de Bioética, (7), 1-15.
5.
Sociedad de Italiana de Anestesia, Analgesia, Reanimación y Terapia Intensiva (SIAARTI) (2020) RACCOMANDAZIONI DI ETICA CLINICA PER L’AMMISSIONE A TRATTAMENTI INTENSIVI E PER LA LORO SOSPENSIONE, IN CONDIZIONI CCEZIONALI DI SQUILIBRIO TRA NECESSITÀ E RISORSE DISPONIBILI.
6.
Beca, J. P., Montes, J. M., & Abarca, J. (2010). Diez mitos sobre el retiro de la ventilación mecánica en enfermos terminales. Rev Med Chile, 138(5), 639-644.
7.
World Health Organization. (2009). Consideraciones éticas en el desarrollo de una respuesta de salud pública a la gripe pandémica (No. WHO/CDS/EPR/GIP/2007.2). Ginebra: Organización Mundial de la Salud.
8.
Gómez Jiménez, J., Ramón-Pardo, P., & Rua Mondaca, C. (2010). Manual para la implementación de un sistema de triaje para los cuartos de urgencias. Washington, DC. Organización Panamericana de la Salud. Organización Mundial de la Salud. OPS/OMS.
9.
Downar, J., Seccareccia, D., & Associated Medical Services Inc. Educational Fellows in Care at the End of Life (2010). Palliating a pandemic: “all patients must be cared for”. Journal of pain and symptom management, 39(2), 291-295.
